-
If you enjoy the forum please consider supporting it by signing up for a NES Membership The benefits pay for the membership many times over.
-
Be sure to enter the NES/MFS May Giveaway ***Canik METE SFX***
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
MA shut down well into June???.....Wife’s work says so.
- Thread starter SgtHal75
- Start date
Mass-diver
NES Member
^good article!
Not looking good....
COVID-19 Projections | US | Massachusetts
We take a data-driven approach rooted in epidemiology to forecast infections, deaths, and recovery timelines of the COVID-19 / coronavirus epidemic in the US and around the world.
covid19-projections.com
Dennis in MA
NES Member
- Joined
- Feb 12, 2007
- Messages
- 38,432
- Likes
- 33,373
I’ll admit, I watch the whole video with the sound off just to see the newscaster...she’s pretty.
Sure. I’d you’re into chicks that look like dudes. Lol. She’s scary looking.
SpaceCritter
NES Member
What's the current wisdom on treating the cytokine storm?We aren’t (from what I have seen) seeing dramatic anemia in these patients which would be an obviously sign of massive red blood destruction.
The elevated ferritin has to do with immune system activation and is linked to the cytokine storm theory related to COVID.
You don’t get a vaccine every year from the flu, you get a flu shot which is a treatment. Why would you get a vaccine every year doesn’t make any sense?..If there was a vaccine for the flu no one would get sick ever.
You're not understanding how the seasonal flu vaccine is formulated.
Please explain to me how a seasonal flu shot is a vaccine? I’m just a simple plain lo’ Marine Veteran and half a hack electrician.You're not understanding how the seasonal flu vaccine is formulated.
Ahhhh the Summer of 2020!!...did all we could to keep from getting heat stroke because we have no A/C and we were stuck inside. I remember it vividly! LolNot looking good....
COVID-19 Projections | US | Massachusetts
We take a data-driven approach rooted in epidemiology to forecast infections, deaths, and recovery timelines of the COVID-19 / coronavirus epidemic in the US and around the world.covid19-projections.com
I went on a doctor’s chat room the other day. The guys there were talking all about guns and bullets.
I think the site was also called NES coincidentally enough. Northeast surgeons or something to that affect. They seemed to know all about guns and stuff. Very interesting.
Thanks
I think the site was also called NES coincidentally enough. Northeast surgeons or something to that affect. They seemed to know all about guns and stuff. Very interesting.
Thanks
Please explain to me how a seasonal flu shot is a vaccine? I’m just a simple plain lo’ Marine Veteran and half a hack electrician.
I think there are a few questions wrapped together here.
I'm not sure how "shot" would be different than "vaccine." I think of "shot" (medically) as a delivery method, not a definition of a type of medical agent. So to me, anything delivered subcutaneously with a needle is a "shot."
Vaccines are a medical preparation that contains dead or weakly effective forms of the virus, and produces an immunity to that disease.
As I understand it, the issues with the seasonal flue vaccine shot are:
1. It's formulated to immunize for the flu viruses that are expected to be most common each year, but production lead times mean the formulation is just an educated (hopefully) guess, so it may or may not be a good fit for what actually develops...if you get exposed to a strain of flu virus that wasn't in the immunization package, it won't help
2. As a sort of meta-problem, there are diseases with "flu-like" symptoms that aren't the flu, and if you get one of those blaming the vaccine for being ineffective is obvious, but might not be accurate
Vaccines formulated for a single virus are far more effective because they're only trying to immunize for that virus (such as small pox, or polio).
Another problem, I think, and I'm not a doc or scientist, is that viruses often mutate, and it seems that the COVID-19 virus is mutating. Logically it seems to me that if it mutates in certain ways, even a vaccine that was highly effective against the version it was developed for might turn out to be weakly effective or not effective at all on mutated relatives of the virus. Just guessing there.
I went on a doctor’s chat room the other day. The guys there were talking all about guns and bullets.
I think the site was also called NES coincidentally enough. Northeast surgeons or something to that affect. They seemed to know all about guns and stuff. Very interesting.
Thanks
What kind of shots were they giving?

babygorilla
NES Member
Except the data is incorrect and makes assumptions. Total infected cannot be quantified without testing 100% of the population for infection or antibodies. Additionally if only 10K die as projected, that is a VERY low percentage of the population of 6.9M. Which, I will point out, they even have the population #'s wrong....Not looking good....
COVID-19 Projections | US | Massachusetts
We take a data-driven approach rooted in epidemiology to forecast infections, deaths, and recovery timelines of the COVID-19 / coronavirus epidemic in the US and around the world.covid19-projections.com
SpaceCritter
NES Member
@Mass-diver since I've been riding my vitamin D hobbyhorse pretty hard: is anyone surveilling for D deficiency in patients?
How I know you didn’t read about their methodology:Except the data is incorrect and makes assumptions. Total infected cannot be quantified without testing 100% of the population for infection or antibodies. Additionally if only 10K die as projected, that is a VERY low percentage of the population of 6.9M. Which, I will point out, they even have the population #'s wrong....
They are independent, the only model shared by the CDC that does not receive government funding.
It’s an AI-based simulation of actual infection rates, not just those tested.
They continually update the model based on local data.
They were one of the first models to suggest really low fatality rate.
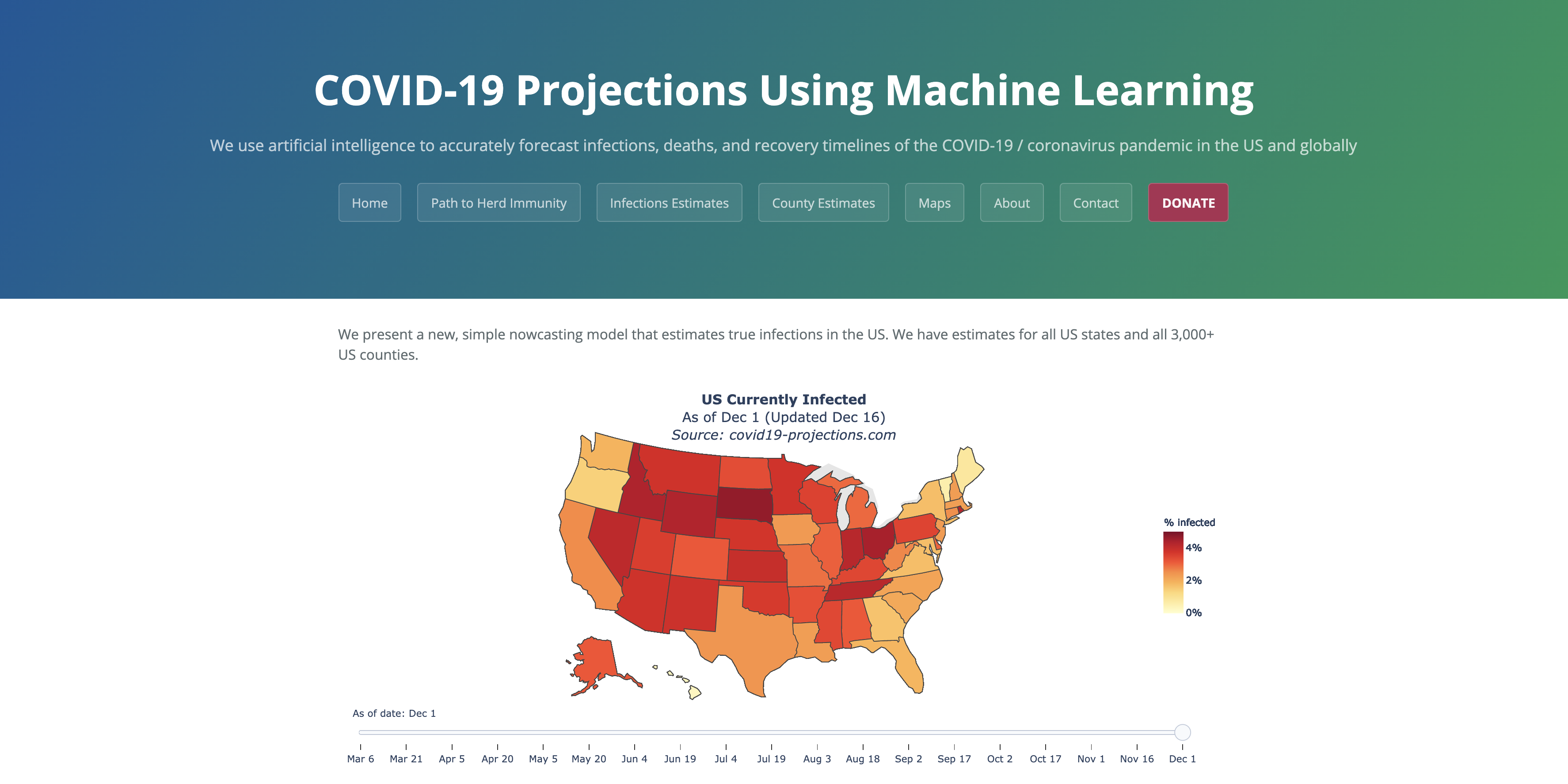
About covid19-projections.com
We use artificial intelligence to accurately forecast infections, deaths, and recovery timelines of the COVID-19 / coronavirus pandemic in the US and globally
covid19-projections.com
Personally, I’m tracking actual deaths and hospitalizations. They’ve both been going down in MA for 5-6 days. My understanding is the restrictions will be lifted when they’ve been going down for two weeks,


What their data shows - and what other countries are already seeing - is that lifting restrictions results in a second jump in numbers. Hoping the May 18 date will stick but this will b3 with us all summer.
It’s called a flu shot not a flu vaccine...I don’t know why this is being questioned???..I know there are other methods of targeting a specific seasonal flu strains like Tamiflu but I laugh at people holding there breath for a vaccine, ain’t happening and of course this thing is going to mutate if not already. Hopefully this Remvisidir shows long term promise for the really sick. Now, for the unhealthy ppl out there who chose a life of bad choices, it’s time to get healthy!!!!!! When this respiratory illness grabs a hold of him it’s not even Covid19 that’s killing them it’s the blood clots in all the other organs. A lot off doctors not on mainstream media (including fox) are not talking about this. Covid 19 could be a blood clot issue more than a respiratory one.I'm not sure how "shot" would be different than "vaccine." I think of "shot" (medically) as a delivery method, not a definition of a type of medical agent. So to me, anything delivered subcutaneously with a needle is a "shot."
SpaceCritter
NES Member
Which countries?What their data shows - and what other countries are already seeing - is that lifting restrictions results in a second jump in numbers. Hoping the May 18 date will stick but this will b3 with us all summer.
I'm not buying their model, FWIW. There are certain things they're not taking into account.
Read the methodology. Oh, then read the methodology. Then read it again. Then show me the model you think is most accurate. What some of you seem to be saying is “I don’t like any model that doesn’t agree with ME!”Which countries?
I'm not buying their model, FWIW. There are certain things they're not taking into account.
Everyone’s an Epidemiologist these days, so your credentials are just as good as Doctors and Scientists who’ve spent their entire careers studying infectious disease and transmission.
SpaceCritter
NES Member
I don't think any of them are, frankly. And the predictions of the so-called experts have turned out to be woefully, horribly wrong.Read the methodology. Oh, then read the methodology. Then read it again. Then show me the model you think is most accurate.
Everyone’s an Epidemiologist these days, so your credentials are just as good as Doctors and Scientists who’ve spent their entire careers studying infectious disease and transmission.
babygorilla
NES Member
My point went over your head. You cannot have an accurate percentage of the population infected without 100% testing. It's called math. What they did is called a guess.How I know you didn’t read about their methodology:
They are independent, the only model shared by the CDC that does not receive government funding.
It’s an AI-based simulation of actual infection rates, not just those tested.
They continually update the model based on local data.
They were one of the first models to suggest really low fatality rate.
About covid19-projections.com
We use artificial intelligence to accurately forecast infections, deaths, and recovery timelines of the COVID-19 / coronavirus pandemic in the US and globallycovid19-projections.com
Personally, I’m tracking actual deaths and hospitalizations. They’ve both been going down in MA for 5-6 days. My understanding is the restrictions will be lifted when they’ve been going down for two weeks, View attachment 353875View attachment 353876
What their data shows - and what other countries are already seeing - is that lifting restrictions results in a second jump in numbers. Hoping the May 18 date will stick but this will b3 with us all summer.
Even the MA.gov #'s are incorrect since they use "presumed" positive in their numbers. And they don't test everyone, intentionally.
babygorilla
NES Member
FIFYWhich countries?
I'm not buying their model, FWIW. There arecertainA LOT of things they're not taking into account.
Why they are calling it a simulator. And why I am tracking deaths and hospitalizations. But those are lagging indicators.My point went over your head. You cannot have an accurate percentage of the population infected without 100% testing. It's called math. What they did is called a guess.//.
Please post up the model you think is most accurate.
Last edited:
babygorilla
NES Member
Since PreCogs don't exist, there is NO guestimate that is accurate unless 100% of the potential data is collected and then the model can be extrapolated. There is NO consistency in how the numbers are obtained. Since the models currently are based on inconsistent quantities (lets count them one way today, no let's count them another tomorrow) and inaccurate numbers (let's guess they have the Wu Flu, lets not test 100% potentials) not have they tested 100% of all potential past infected (antibodies)Read the methodology. Oh, then read the methodology. Then read it again. Then show me the model you think is most accurate. What some of you seem to be saying is “I don’t like any model that doesn’t agree with ME!”
Everyone’s an Epidemiologist these days, so your credentials are just as good as Doctors and Scientists who’ve spent their entire careers studying infectious disease and transmission.
babygorilla
NES Member
No guess is ever accurate without accurate numbers. I don't make estimates based on half baked numbers that inconsistently applied and on half truths. So far there is NO way to even model this, since they can't even agree on who is positive or not.Why they are calling it a simulator. And why aim tracking deaths and hospitalizations. But those are lagging indicators.
Please post up the model you think is most accurate.
kevin9
NES Member
May be a better model, structurally speaking, but GIGO. Given the way authorities have been manipulating and massaging the reported data I'd be hesitant to make any model-based decisions without significant normalization and cleaning of the input data.Not looking good....
COVID-19 Projections | US | Massachusetts
We take a data-driven approach rooted in epidemiology to forecast infections, deaths, and recovery timelines of the COVID-19 / coronavirus epidemic in the US and around the world.covid19-projections.com
Also note this particular model appears to be a one-man-band, Youyang Gu of NYC.
babygorilla
NES Member
EXACTLY!May be a better model, structurally speaking, but GIGO. Given the way authorities have been manipulating and massaging the reported data I'd be hesitant to make any model-based decisions without significant normalization and cleaning of the input data.
How did I know Trump was going to win, I looked at the numbers at the rallies in comparison (T vs. H) and the # of bumper stickers.
How do I know many of the numbers of Kung Fu Flu are BS? I look at people NOT REALLY sheltering in place, and how few are really affected, and how the media and the PtB change the accounting to try to make themselves not look bad. And their retiscence to test. When they are ONLY testing what they BELIEVE to be 100% infected persons, and only 25% end up being actually positive, that tells you that the numbers af actual infected are significantly lower, coupled with the fact they started COUNTING suspected infected as positives once those tests started coming back negative and that fact became known.
Also known as reading between the lines.....
Dennis in MA
NES Member
- Joined
- Feb 12, 2007
- Messages
- 38,432
- Likes
- 33,373
What kind of shots were they giving?
Half 9mm. The other half, .45.
kevin9
NES Member
FYI. Here's a comparison of 3 major sources of COVID-19 data: COVID-19 deaths and cases: how do sources compare?
And here's the list of known issues with the JHU CSSE data: CSSEGISandData/COVID-19
IMNSHO there's not good data set (yet). Too much of the reporting has been skewed by multiple factors in different directions (ex. deliberate under-reporting, over-reporting deaths, variable degree of infection and anti-body testing, etc). All the data sources are going to be crap until those factors can be accounted for.
And here's the list of known issues with the JHU CSSE data: CSSEGISandData/COVID-19
IMNSHO there's not good data set (yet). Too much of the reporting has been skewed by multiple factors in different directions (ex. deliberate under-reporting, over-reporting deaths, variable degree of infection and anti-body testing, etc). All the data sources are going to be crap until those factors can be accounted for.
No guess is ever accurate without accurate numbers. I don't make estimates based on half baked numbers that inconsistently applied and on half truths. So far there is NO way to even model this, since they can't even agree on who is positive or not.
Very good observation. A fundamental principle in epi research is the homogeneity of disease events identified by the researcher. Given the yuuuuge incentive for financially strapped hospitals to upcode everything to a Covid death, and the unreliability of tests, my opinion as a scientist is that the model outputs are suspicious.
Having said that, policymakers are just going to pick (and fund) whichever model is convenient for them to enact the policies they want to enact anyways. I have seen the sausage-making. Scientific findings are political weapons.
SpaceCritter
NES Member
The one thing I will say is that the Worldometer numbers for Connecticut match what's been coming out of the governor's office.FYI. Here's a comparison of 3 major sources of COVID-19 data: COVID-19 deaths and cases: how do sources compare?
And here's the list of known issues with the JHU CSSE data: CSSEGISandData/COVID-19
IMNSHO there's not good data set (yet). Too much of the reporting has been skewed by multiple factors in different directions (ex. deliberate under-reporting, over-reporting deaths, variable degree of infection and anti-body testing, etc). All the data sources are going to be crap until those factors can be accounted for.
Share:
Similar threads
- Replies
- 16
- Views
- 1K